Demographic and economic trends, combined with the sheer magnitude of the unmet needs in the emerging markets represents the largest untapped opportunity for advanced wound care products and services globally.
Introduction
As the business of advanced wound care in North America and Western Europe has boomed for the past two decades, most major wound care product and services firms, which are overwhelmingly based in those markets, have made comparatively little investment in the developing world.
To be clear, the complex wound epidemic in the developed world is far from over, and it will remain a high growth healthcare opportunity for years to come. Yet trends such as new market entrants, insurance consolidation, increasingly cumbersome documentation requirements, and the commoditization and market saturation of certain product types, combined with overall pressures to cut healthcare costs, have at a minimum impacted per-unit/per-patient profitability in the West, even as the total market size continues to soar. Emphasis on prevention, bundled payments, and other risk-sharing trends on the horizon will further challenge the lucrativeness of wound care in the developed markets.

At the same time, aging populations, wound-related comorbidities, and increasing purchasing power and overarching demand for advanced healthcare in the emerging and frontier markets have created tremendous opportunities for specialized wound care in these regions. Of course, unique challenges and obstacles exist as well. Still, demographic and economic trends, combined with the sheer magnitude of the unmet needs in the emerging markets represents the largest untapped opportunity for advanced wound care products and services globally. In line with this, greater than 50% of our 2016 engagements and related advisory at Diligence Wound Care Global involved the emerging and frontier markets. This trend has continued into 2017 as well.
In this article, we will explore:
- The current state of advanced wound care across the developing world.
- Global demographic and financial data, cultural-religious considerations, and real-world, on-the-ground international wound care experience and information I have gathered from my wound care colleagues and during my extensive travels.
The reader will gain a keener appreciation of evolving opportunities for wound care (and other healthcare) executives, specialists, startups, and investors.
Why look to the emerging markets for wound care?
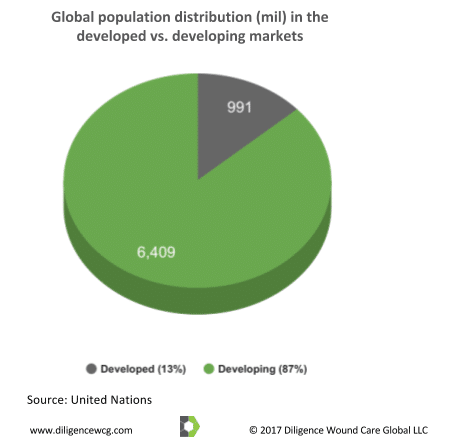
With between 6 to 7 million complex wounds, estimated market sizes of between USD $8bil to $15bil for advanced wound care products, and $40bil to $60bil for wound management-related services in the United States alone (depending on which specific wound etiologies, products, and services are included), why should executives and investors even consider placing valuable resources in the emerging and frontier markets? The following figures provide an answer:
1. Population size and distribution
2. Overweight, obesity, and other malnutrition
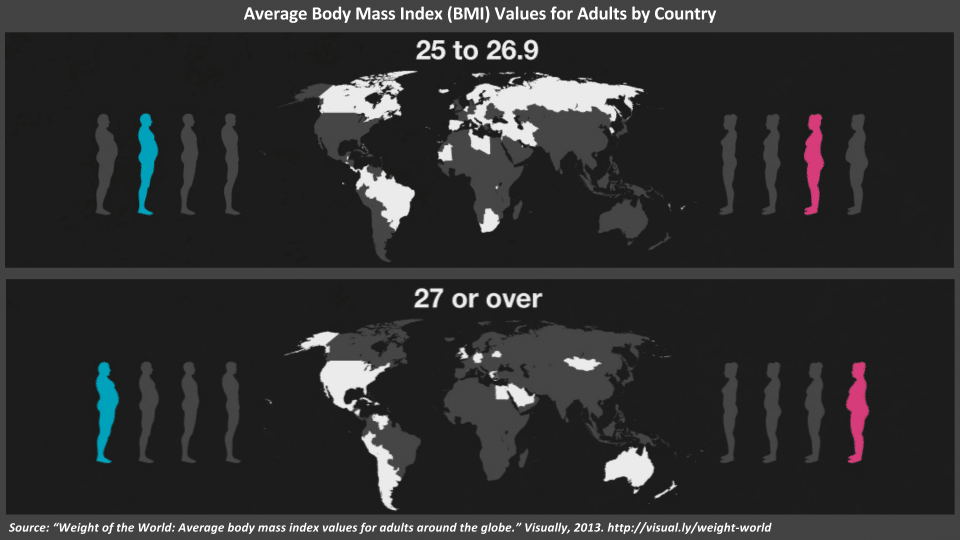
As if overweight and obesity were not enough of a challenge, due to evolving demographic, economic, and cultural factors affecting diets (e.g. urbanization, a shift to processed foods, etc.), many emerging markets have simultaneously overweight/obese yet undernourished populations. The lack of protein, micro-nutrients, and other consequences–even as average BMIs soar–is yet another comorbidity associated with delayed wound healing. This phenomena is well-documented in the 2016 World Bank paper, The Double Burden of Malnutrition in East Asia and the Pacific: Evidence and Lessons for a Multisectoral Response.
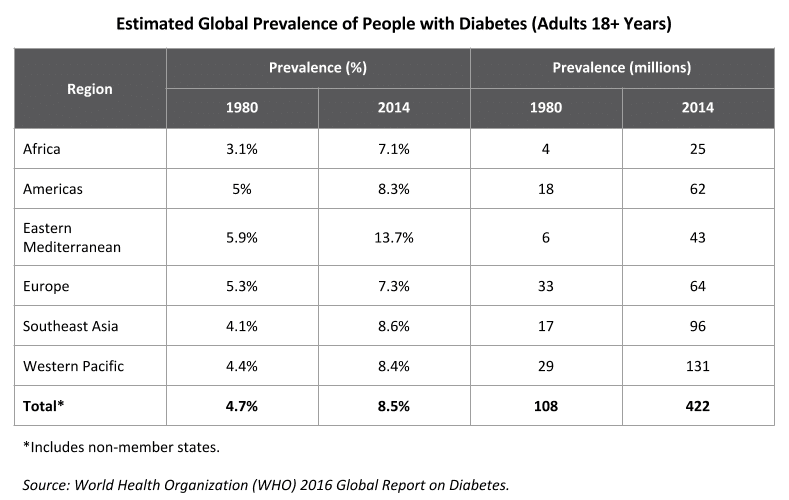
3. Diabetes
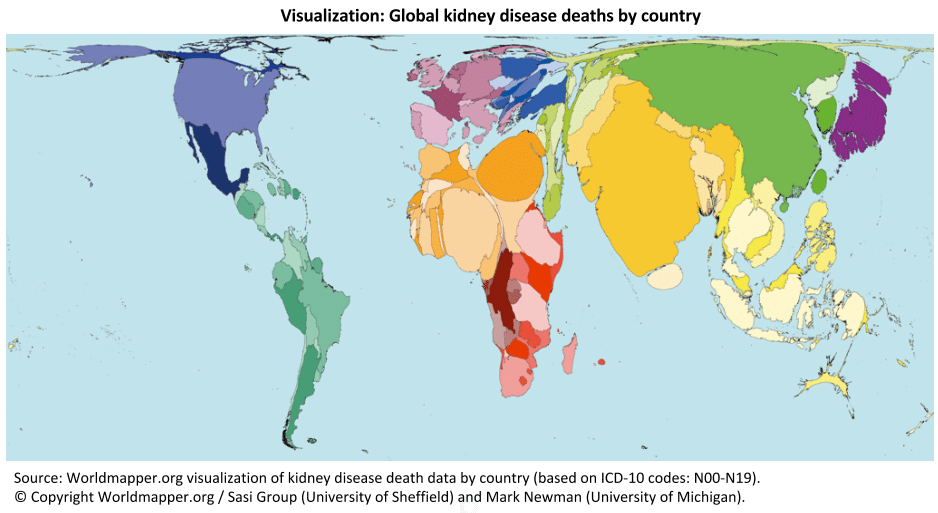
4. Kidney disease
5. Smoking
Despite an overall reduction in smoking across the developed markets, 80 percent of the world’s 1 billion smokers are in low and middle income countries (WHO), with double-digit increases in smoking rates across dozens of developing nations. Indonesia alone is home to 70 million smokers, a nearly 30 percent increase over 15 years. During the same period, the percentage of Jordanian smokers rose from 25 to 40 percent. Similarly, rates in Bahrain rose from 12 percent to almost 30 percent, and in Cameroon from 7 percent to 22 percent. The CDC reports that overall, smoking in the developing world is increasing at a rate of 3.4 percent annually.
As anyone who has worked in wound care services knows, smoking (and the resulting cardiovascular and pulmonary complications) is one of the most difficult clinical challenges faced by the wound care provider. While for most patients (in theory), wound bed moisture can be balanced, microbial counts (infections) reduced, albumin/pre-albumin levels raised, and blood glucose controlled, the damage that years of smoking does to the body’s ability to deliver oxygen required by healing tissue is extremely difficult to reverse in both the short and long terms. Noninvasive therapies to improve tissue perfusion are only effective if there is a certain amount of underlying vascularization. Yet invasive revascularization procedures are both medically complex and financially costly. In this sense, the colossal, growing rates of smoking in many of the world’s developing nations simultaneously contributes to both the clinical challenges and business opportunities for advanced wound care in these markets.
The connection to chronic wounds
Thanks to firms such as Net Health, it is possible to access real-time data comparing the effects of both individual and multiple comorbidities on wound healing. Such data is sourced from hundreds of thousands of wound outcomes across hundreds of US wound care centers. The following figures show that the chronic diseases and related factors that plague the developing markets are precisely the ones that have the most profound impacts on delayed wound healing:
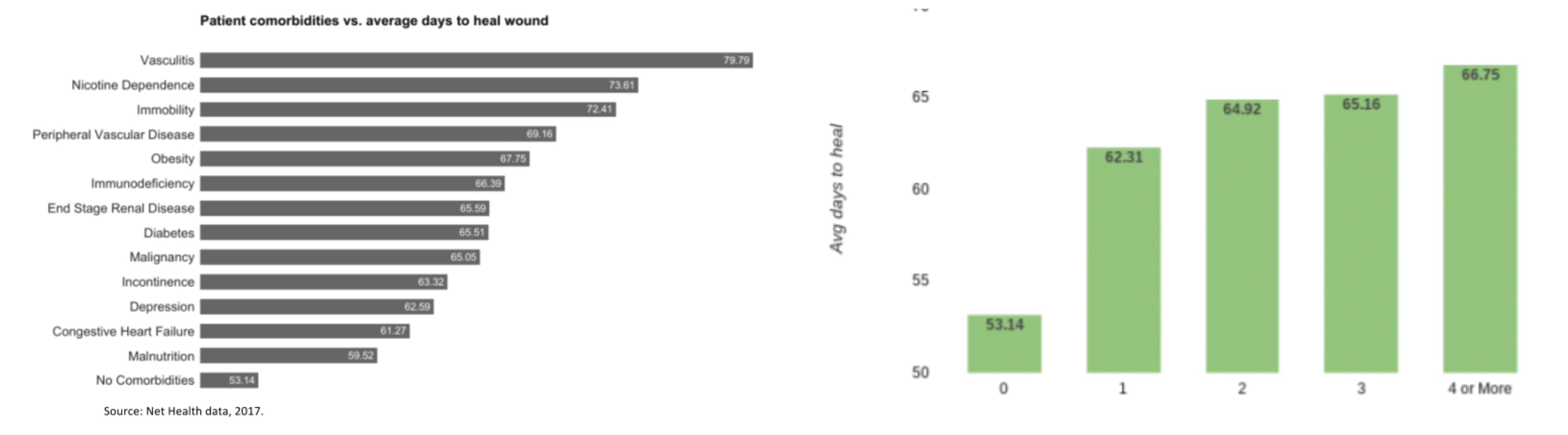
The comorbidities found to have the most acute impacts on patients in the US are also the most prevalent and fastest growing conditions in the emerging markets.
Clearly, from the perspectives of both absolute and relative population sizes, as well as factors associated with non-healing wounds, the current and future needs in the developing world are immense. As we will see, despite these figures, specialized wound care in these regions has traditionally been the focus of disproportionately low levels of investment. We will dive deeper into just how massive the opportunities are in future articles and posts.
Wound care products and services: “Chicken-and-egg?”

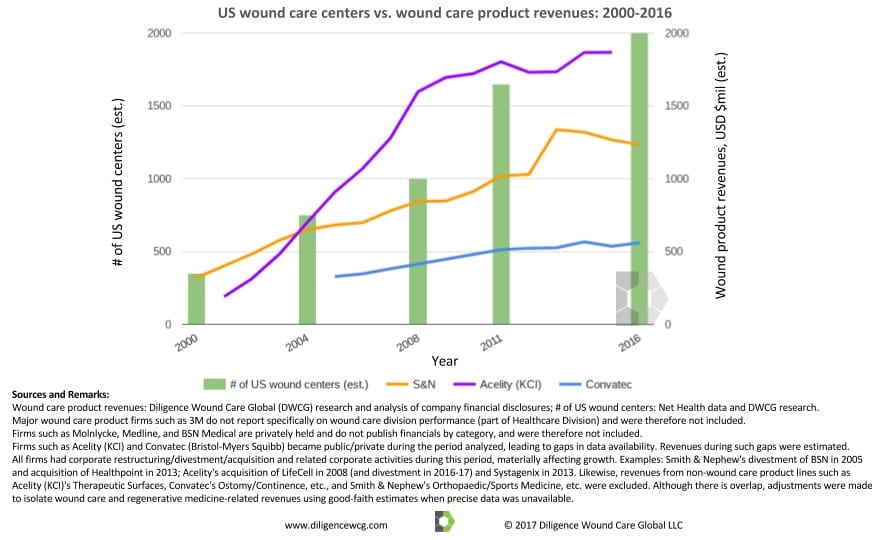
Which should come first–emerging market wound care products, or services? Having been first introduced to advanced wound care in the developed markets (as a director for a leading wound management firm), I had always been exposed to a plethora of advanced therapies, as well as adequate facilities and providers to utilize them. Yet over the past 20 years, the growth of wound care product revenues in the US has been strongly correlated with the burgeoning of specialized wound care services.
Many industry veterans with whom I spoke linked the massive increase in US wound care centers during this period to the increase in US hyperbaric oxygen therapy (HBOT) as a result of favorable reimbursement and related trends since the early 2000s (growth of HBOT utilization has recently been challenged, largely due to new documentation requirements and related audits). In their recollection, hospitals and clinics had incentives to launch stand-alone HBOT service lines, initially investing in wound care centers primarily as a way to source patients for HBOT. The increase in wound care centers in turn drove the development and utilization of advanced products (and with them, increasingly lucrative procedures), which in turn continued to fuel the growth of wound management firms and overall awareness and education within the market. Combined with the clear and growing clinical need, the result was a 570% increase in the number of US wound centers from 2000 to 2016.
The following chart illustrates the relationship between the growth of US wound care services and product revenues among the leading firms (which are overwhelmingly derived from US sales):
Through my travels and research I have found that many versions of advanced wound care products exist across the globe, even as relatively few patients can access them. In fact, while there are certainly fewer product options available, most major categories of wound care products (or an improvised version) are available in the emerging markets should a healthcare provider wish to utilize them.

From my experience in the emerging and frontier markets, while many wound care products still have a long way to go to achieve ubiquity, it is the lack of specialized wound care services (wound care centers, home health, rehabilitation centers, etc.) that tends to be the limiting factor for patient access to modern wound care modalities. The following chart illustrates the vast disparity between the number of wound care centers relative to the populations of the US vs. several emerging markets:
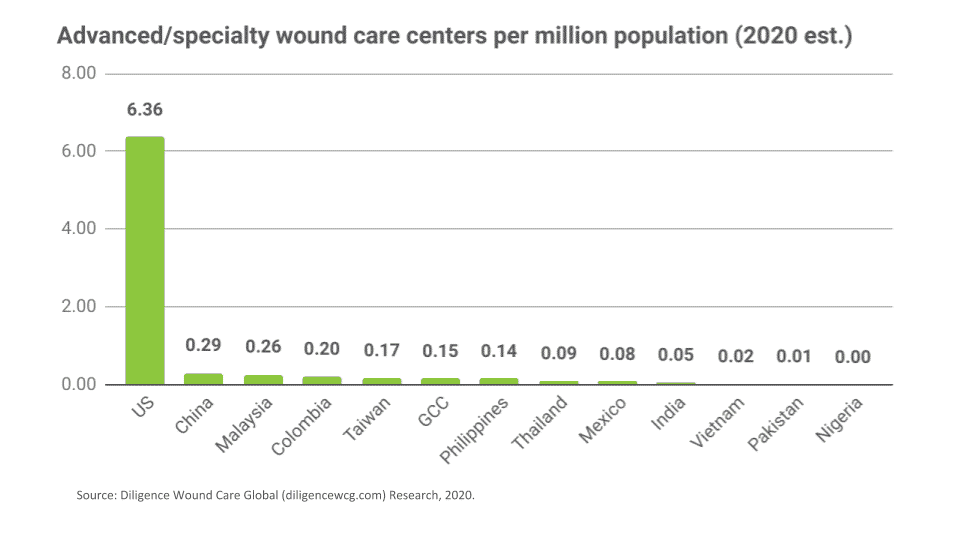
Even in markets where per capita advanced healthcare significantly infrastructure lags the US, the lack of wound care infrastructure is disproportionately high. While it is understandable that access to specialized wound care treatments is not as available in the developing markets as in the developed markets, it is evident that this disparity is more immense than might be expected–even when compared to the relative availability of other categories of advanced medical treatments across the same areas (and is therefore a business opportunity).
Cultural-Religious Emerging Market Wound Care Considerations

We would be remiss to discuss wound care in the developing world without mentioning the cultural-religious considerations and needs of such markets. Although little, if any, academic literature exists on this topic, anyone who has been involved in emerging market wound care understands that cultural-religious challenges is a relevant aspect that must be considered.
Theravada Buddhist Diets and Routines

One cultural-religious need associated with chronic wounds can be seen in regions with many Theravada Buddhists, of which there are an estimated 150 million to over 230 million globally. Countries such as Laos, Myanmar (Burma), Thailand, Cambodia, and Sri Lanka have particularly large concentrations. Bangladesh, China, India, Nepal, Vietnam, and other countries also have significant Theravada populations. Theravada monks number in the millions, but the precise number is difficult to quantify because most Theravada Buddhist men spend part of their lives as monks, ranging from several days to many years. Theravada monks are an example of a group recently at high risk for chronic wounds as a result of cultural-religious practices combined with the emerging market chronic illness trends discussed above.
A recent study found that nearly half of Thailand’s 300,000 monks are obese, with 42 percent having high cholesterol, 23 percent hypertensive, and more than 10 percent diabetic (the prevalence of overall adult diabetes in Thailand is 8 percent). According to Jongjit Angkatavanich, a Thai health and nutrition expert, “Obesity in our monks is a ticking time bomb.”
I discussed this data with wound care providers in Theravada Buddhist regions, and they overwhelmingly confirmed that a disproportionately large number of their patients suffering from diabetic foot ulcers (DFUs) are monks. Given the multiple risk factors documented above, this makes sense. Some cultural-religious aspects that might explain this trend include:
- Theravada monks spend most of their time relatively sedentary (much of their typical day is spent in meditation and prayer).
- They perform “alms rounds,” where they leave the temple in the early morning, and accept gifts of food as their first meal of the day (since they are prohibited from collecting material things, including food), which often consist of sweet rice and dessert items, as well as sugary drinks.
- During alms rounds (and for most of the day), the monks are barefoot, which of course increases the likelihood of wounding events. When not barefoot, monks wear thin sandals, which are also likely to cause or complicate wounds, especially in diabetic, overweight, and/or older individuals.
- Some monks eat only once per day, with others eating twice per day, causing spikes in blood glucose levels that affect A1C levels (leading to or exacerbating diabetes, heart disease, and other chronic wound-related complications).
- Additionally, they must finish their final meal before mid-day, leading to additional difficulty in controlling swings in blood sugar, a key element involved in prevention of neuropathy and other lower leg complications associated with diabetes.
- Likewise, monks are neither allowed to hoard food nor cook. There are also certain foods that are prohibited for monks during certain times of the day (ironically, sugar, honey, and syrup are permissible at any time), all of which contribute to nutritional risks such as protein deficiencies and uncontrolled diabetes that are associated with non-healing wounds.
Middle Eastern/Central Asian Footwear and Sitting Position

Another cultural-religious trend relevant to the topic of wound care in the emerging markets relates to majority Muslim countries, particularly in The Middle East. In preparing this article, I spoke with Dr. Lee Rogers, a wound care provider, management executive, and Managing Partner at The Amputation Prevention Experts (APEx) Network, which provides medical training and case management services for the prevention and treatment of diabetic foot complications.
At the time Dr. Rogers and I spoke, he was literally in transit back to the US after a visit to the Persian Gulf, a region where multiple countries have diabetes rates exceeding 25 percent of the adult population. Bahrain, Kuwait, Qatar, Saudi Arabia, and the United Arab Emirates are all ranked in the top 15 most obese countries.
According to Dr. Rogers, “They’re going to see a tsunami of amputations…it’s almost like diabetes caught them by surprise.” There is scientific evidence supporting this prediction as well. In a 2012 article entitled, “Diabetes-Related Lower Extremities Amputations in Saudi Arabia: The Magnitude of the Problem” published in the Annals of Vascular Diseases, Saudi surgeon Dr. Hasan Ali Alzahrani analyzed known in-country data against global projections, concluding that, “Half a million diabetes-related amputations of the lower extremities are likely to occur in…MENA [Middle East and North African] countries over the coming decade.”
According to a Wall Street Journal article on the diabetes epidemic in that region, “Unhealthy lifestyles and urbanization are to blame—particularly in the Persian Gulf where the discovery of oil has created wealth that has decreased physical activity, according to doctors and analysts.”
While high a prevalence of diabetes, obesity, smoking, inactivity, and other risk factors is associated with chronic wounds and lower extremity amputations, none of these are cultural-religious issues unique to either The Middle East region or the Muslim religion. However, they lay the groundwork for such issues to create wound-related problems. Specifically, Dr. Rogers and I discussed these examples of specific cultural-religious phenomena in these populations that exacerbate the problem:
- Traditionally, many Muslims choose to sit cross-legged, especially when eating or socializing. This custom is considered a sunnah (a practice by the prophet Muhammed, which Muslims seek to emulate). As a result, “the healthcare providers I met with told me they see disproportionate numbers of wounds on the lateral malleolus [outer ankle],” Dr. Rogers explains. While pressure, friction, and shear resulting from such a sitting position would not normally cause a wound in healthy adults, the staggering rates of regional comorbidities has transformed such an innocent activity into a contributing factor for a health epidemic. (Note: many Indians and other cultures also commonly sit on the floor in a similar fashion, especially during meals. Some of the stated benefits include improved digestion, flexibility and posture, mindful eating, relaxation, and heart strength. While I have not yet seen or heard of wound-specific issues in those populations to date, it is reasonable to suspect that this could be a relevant factor for them, too).
- Many men (and more recently women) in The Gulf Region wear a particular style of sandal called madas or madas sharqi (literally “sandal from the east”), with a leather loop surrounding the great toe (hallux), as depicted in the image below. This can lead to abrasions and other footwear injuries, which combined with other risk factors, may progress to stalled wounds which can quickly escalate to infections and amputations.
- Wearing sandals in general (regardless of style), combined with the regionally hot and dry air, as well as walking barefoot on hot sand or other potentially traumatic surfaces (such as removing footwear prior to praying) can lead to cracked, torn, blistered, or burned skin that too may progress into a chronic wound if not screened and treated early.
As a result of the factors described above, the amputation rate for diabetic foot ulcers (DFUs) in at least one hospital in this region is upwards of 60 percent.
Traditional Eastern Medicine

Many cultures, particularly across Asia, emphasize herbal and other alternative therapies (Eastern Medicine). Evidence does indeed exist proving the clinical benefit of many of these therapies (such as massage and acupuncture for relieving certain types of pain), but a common critique of alternative modalities is that most lack robust assessments of clinical efficacy and effectiveness such as randomized controlled trials (RCTs). As summarized by the US NIH official page on Traditional Chinese Medicine (TCM), “For most conditions, there is not enough rigorous scientific evidence to know whether TCM methods work for the conditions for which they are used.” While certain supplements and teas may indeed for example, relax pressure around blood vessels (thereby potentially improving circulation), many of them have side effects or unintended drug interactions that can have negative overall consequences. Of equal importance, a potentially beneficial alternative remedy used in lieu of proven wound care prevention and treatment modalities can be problematic, especially as time is not on the side of the patient with a stalled wound (an herbal remedy to improve circulation is not going to reverse a gangrenous arterial toe ulcer).
Still, alternative treatments can have a role in wound care, particularly in the emerging markets. In fact, in most Asian nations with national healthcare schemes, many Eastern therapies are partially or fully covered. Elements of traditional medicine can be leveraged by wound care stakeholders in the markets we are discussing in the following ways: 1) as adjunctive clinical therapies, 2) to improve patient compliance and satisfaction, and 3) as drivers of direct and indirect revenues for wound care product and service firms. We will further explore these prospects in future content.
Other Ethno-cultural wound care considerations
In multiple regions, other cultural-religious sensitivities surrounding certain wound care products and services exist as well, including:
- Porcine (pig) derived products, like in many medical and surgical specialties, are commonly used in advanced wound care. This includes certain collagen dressings, allografts (such as extracellular matrices/ECMs), and the emerging, exciting category of hemoglobin oxygenizers. While many clerics and religious leaders maintain that the prohibitions against such products do not apply to certain medical uses, at a minimum, the regulatory approval process, clinical education, and patient/provider decision making processes are impacted by such considerations. Bovine (cattle), equine (horse), sheep (ovine), and other animal (especially mammal)-derived products may also cause objections. For instance, some patients and providers might expect that the animal from which the product is sourced meet the halal dietary restrictions of the Muslim religion.
- Certain markets may have issues with any type of human or animal product usage, regardless of the species it is derived from. An Asian producer and distributor of a topical human growth factor (HGF) for wounds once lamented to me that while the providers with whom he spoke were eager to use the product, its launch had been delayed by over a year in Thailand (93% Buddhist, 6% Muslim) due to cultural-religious regulatory approval delays.
- I was recently invited to participate in a panel during a forum in Bangkok for wound care leaders in Southeast Asia. The event was part of a soft launch for an extremely innovative product containing porcine (pig) derived molecules. The attending healthcare providers from across the region were extremely impressed with the product’s scientific evidence and practical ease-of-use. Still, wound care providers from Malaysia and The Philippines (Indonesian providers did not attend this particular event) were concerned that significant portions of their patient populations might have an aversion to the product, despite its clear medical benefit and reasonable cost.
- On a similar note, a Vietnamese medical distributor I recently met with in Ho Chi Minh City asked me if I could connect them with a coral-derived bone grafting supplier with whom I am in touch. Although most high-quality bone grafts are traditionally sourced from human or animal sources, stakeholders in that market, who primarily practice a mixture of Vietnamese indigenous folk religions, Buddhism, and related combinations of Confucianism and Taoism, were demanding higher quality, non-animal derived, non-synthetic substitutes, which created a market opportunity.
- When I directed wound care centers in the US, we would occasionally treat patients from Sub-Saharan Africa and The West Indies (as either medical tourists or patients who immigrated to the US later in life). Many of these patients, especially the older ones, were adamant that their wounds would not heal due to evil spirits or curses. In between wound center visits (or even during hospitalizations), they would attempt remedies recommended by shamans or witch doctors. Some involved removing dressings or tampering with the wound bed. Clinicians treating these populations needed to diplomatically handle such sensitivities to maximize patient compliance. For example, rather than ordering the patients to do nothing in between visits, one physician I worked with would encourage the patient to focus on the neutral/harmless remedies instead of the harmful ones.
In short, diligent wound care executives and investors should factor the potential impact of cultural-religious considerations into their market assessments and commercialization plans when launching wound care products in the emerging markets. Planning and budgeting for regulatory approval timelines (and risks), as well as a candid assessment of the TAM (Total Available Market) and SOM (Serviceable Obtainable Market) is just as important when executing business strategy in the emerging markets as it is in the mature markets. In like manner, these same cultural-religious “obstacles” can also be leveraged by innovative wound care and regenerative medicine firms to address unique emerging market opportunities, an idea we will discuss later in this article series.
Conclusion

In this article, we discussed:
- the significant gap in wound care infrastructure between the developed vs. developing markets,
- unmet present and future demographic and population health needs in these regions, and
- relevant cultural-religious influences associated with complex and non-healing wounds in the emerging markets.
An overarching theme in emerging market wound care is the huge imbalance of need vs. access / infrastructure, even more so than most other healthcare sub-specialties. As with any such disparity, this creates tremendous opportunities for forward thinking executives, investors, and clinicians.
Are you an executive or investor with experience in emerging market wound care launches, management, or an interest in particular challenges and opportunities in these regions?
Are you a clinician who has been involved in wound care treatment, research, or training in the developing world?
Please share your thoughts in the comments below, or contact us to discuss.
Global Advanced Wound Care Market was valued at USD 9.45 billion in 2020, growing at a CAGR of 10.51% during the forecast period from 2021 to 2026, to reach USD 16.97 billion by 2026 | Estimated by Delveinsight
View Here: https://www.delveinsight.com/report-store/advanced-wound-care-market